Home / Dafeepedia/ What Is Cholesterol?
What Is Cholesterol?

What Is Cholesterol?
Cholesterol is a lipid molecule — more precisely a sterol — present in every cell of the human body. It is not a dietary fat. It is not a poison. It is a structural molecule essential to life.
The body synthesises cholesterol across multiple tissues. The liver is the primary site of endogenous production, but cholesterol synthesis also occurs in the intestines, adrenal glands, skin, and reproductive tissues. Estimates suggest the liver accounts for approximately 70–80% of total endogenous synthesis, though this varies by individual and metabolic state.
Dietary cholesterol contributes a variable proportion of whole-body cholesterol balance. Intestinal absorption efficiency differs substantially between individuals, and endogenous synthesis adjusts dynamically in response to dietary intake — a regulatory mechanism known as compensatory down regulation.
This distribution illustrates a fundamental point: cholesterol is so necessary to normal physiological function that the body maintains dedicated biosynthetic pathways across multiple organ systems, independent of dietary intake.
Because cholesterol is poorly soluble in water, it circulates packaged within lipoproteins such as LDL, HDL, VLDL, IDL, and lipoprotein(a). These particles serve as transport vehicles, carrying cholesterol and triglycerides through the bloodstream to tissues throughout the body.
Complete guide to reading your cholesterol results
What Does Cholesterol Actually Do?
Cholesterol fulfils five essential biological roles: it regulates cell membrane fluidity, serves as the precursor to all steroid hormones (estrogen, testosterone, cortisol), enables vitamin D synthesis in the skin, is converted by the liver into bile acids for fat digestion, and plays a structural role in brain myelin sheaths and synaptic function.
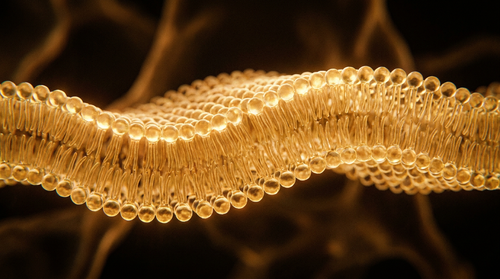
Cell membrane structure
Every cell in your body is surrounded by a membrane partly composed of cholesterol. It regulates membrane fluidity and permeability — a balance that is necessary for normal cellular function. [SOURCE: cell biology — Alberts, Molecular Biology of the Cell]
Hormone synthesis
Cholesterol serves as the precursor for steroid hormone synthesis. Adequate cholesterol availability is necessary for the production of cortisol, aldosterone, testosterone, oestrogen, and progesterone. [SOURCE: endocrinology — Guyton and Hall, Medical Physiology]
Vitamin D
The synthesis of vitamin D — technically a hormone — begins with cholesterol in the skin, activated by UVB rays.
Bile acids
The liver converts cholesterol into bile acids, which are necessary for the digestion and absorption of dietary fats and fat-soluble vitamins (A, D, E, K).
Neurological function
A substantial proportion of the body's total cholesterol is found in the brain, where it plays a structural role in myelin sheaths and contributes to synaptic function. [SOURCE: neurology — Björkhem and Meaney, Arteriosclerosis, Thrombosis, and Vascular Biology, 2004] Note: brain cholesterol is largely synthesised locally by glial cells and is largely independent of circulating plasma cholesterol due to the blood-brain barrier.
Why Did We Fear Cholesterol?
The fear of cholesterol originates from the 1950s work of Ancel Keys and his Seven Countries Study, which observed a correlation between saturated fat consumption, blood cholesterol levels, and cardiovascular mortality. This contributed to decades of public health messaging that simplified a complex relationship into a single directive: lower your cholesterol. [SOURCE: Keys A. et al., Seven Countries Study, 1970]
Keys observed a correlation between saturated fat consumption, blood cholesterol levels, and cardiovascular mortality across seven countries. His findings contributed to what became known as the diet-heart hypothesis — the idea that dietary fat raises blood cholesterol, which in turn increases cardiovascular risk.
This hypothesis shaped global nutritional guidelines for decades. By the 1980s, the message had been simplified into a public health directive: reduce fat, lower cholesterol, reduce heart disease risk.
The scientific reality was more complex. The Seven Countries Study has been both influential and contested. Critics have argued that the selection of countries and the methodology introduced biases into the conclusions. [SOURCE: Yerushalmy J, Hilleboe HE, NY State J Med, 1957] However, many of these critiques have themselves been challenged — the popular claim that Keys deliberately excluded contradictory data is considered by several historians of science to be an oversimplification of a more nuanced methodological debate.
What is broadly accepted today is that the diet-heart hypothesis, while not entirely wrong, was applied too broadly and too uniformly. The relationship between dietary fat, blood cholesterol, and cardiovascular risk is mediated by the type of fat consumed, the type of lipoprotein carrying the cholesterol, individual metabolic context, and genetic factors — none of which a single population study could fully capture.
The simplification was not necessarily intentional. It was the product of translating complex epidemiology into actionable public health policy — a translation that inevitably loses nuance.
Why is total cholesterol not enough to assess cardiovascular risk?
Total cholesterol is an aggregated value that adds together all circulating lipoprotein fractions — LDL, HDL, and estimated VLDL.
Two people with an identical total cholesterol of 200 mg/dL can present radically different cardiovascular profiles depending on how that total is distributed across these fractions. [SOURCE: Friedewald WT et al., Clin Chem, 1972]
Total cholesterol alone does not tell you who is carrying the cholesterol, in what form, or toward which tissues. It is a sum without decomposition.
The markers that add meaningful information:
ApoB — measures the total number of circulating atherogenic particles, independent of their cholesterol content. Two people with the same LDL-C can have very different ApoB concentrations. [SOURCE: Sniderman AD et al., JAMA Internal Medicine, 2019]
Triglyceride/HDL ratio — a ratio above 3 (in mg/dL) is associated with insulin resistance and a predominance of small dense LDL particles, the most atherogenic form. [SOURCE: McLaughlin T et al., Circulation, 2003]
Lipoprotein(a) — a distinct particle, genetically determined, not modifiable by diet. An independent cardiovascular risk factor not captured by a standard lipid panel. [SOURCE: Nordestgaard BG et al., European Heart Journal, 2010]
When Does Cholesterol Actually Become a Problem?
Cholesterol becomes a cardiovascular risk factor when LDL particles are small and dense, oxidised, or present in high numbers — not simply when total cholesterol exceeds a threshold. Small dense LDL penetrates arterial walls more easily and oxidises more rapidly than large buoyant particles, even at identical LDL-C concentrations.
Small dense LDL particles are more atherogenic than large buoyant particles, even at identical LDL-C concentrations. They penetrate the arterial wall more easily and oxidise more rapidly. [SOURCE: Austin MA et al., JAMA, 1988]
Oxidised LDL — not native LDL — is the form implicated in atherosclerotic plaque formation. LDL oxidation is promoted by chronic inflammation, smoking, and oxidative stress. [SOURCE: Steinberg D et al., NEJM, 1989]
Elevated ApoB — independent of LDL-C — predicts cardiovascular risk more accurately in several cohort studies. [SOURCE: Sniderman AD et al., Lancet, 2006]
The overall metabolic context — insulin resistance, hypertension, systemic inflammation (CRP), physical inactivity — amplifies lipid risk. A moderately elevated LDL in a healthy metabolic context presents a different risk profile than the same LDL in the context of metabolic syndrome.
Real risk is not in a number. It is in the pattern formed by all the markers together.
Low Cholesterol: Is It Always Good News?
Very low cholesterol is not automatically a marker of optimal health. Some observational studies report associations between very low cholesterol concentrations and neurological and hormonal outcomes, though these findings remain debated and do not establish causation. The well-established benefits of LDL reduction in high-risk populations are not in question — individual metabolic context determines interpretation.
Similarly, some meta-analyses have examined the relationship between very low LDL concentrations and haemorrhagic stroke risk, with mixed findings. This remains an area of active research without definitive consensus.
On the hormonal side, cholesterol serves as the biochemical precursor for steroid hormone synthesis. Whether circulating LDL concentrations at the lower end of the clinical range meaningfully affect hormone production in otherwise healthy individuals is not established with certainty and likely depends on individual metabolic context.
The well-established benefits of LDL reduction in high-risk cardiovascular populations — particularly through statin therapy — are not in question here. [SOURCE: Collins R et al., Lancet, 2016 — Cholesterol Treatment Trialists] The point is more limited: very low cholesterol is not automatically a universal marker of optimal health, and clinical interpretation should always account for individual context.
What Your Lipid Panel Is Really Telling You
A lipid panel reveals your complete lipid metabolism profile — not just isolated numbers. The pattern formed by LDL, HDL, triglycerides, non-HDL cholesterol, and the TG/HDL ratio together contains more clinical information than any single marker in isolation. Ratios and interactions between markers define real cardiovascular risk.
This is precisely what the Dafee Lipid Intelligence engine does: it identifies the pattern formed by your markers, classifies it among ten distinct metabolic profiles, and translates that pattern into plain language — without replacing your doctor, without making a diagnosis, but giving you the interpretive framework that a standard consultation does not have time to provide.


Written by the Dafee Science Team — published 17/05/2026. Dafeepedia content is developed from peer-reviewed scientific literature and European regulatory sources, and reviewed for accuracy before publication.
The Dafee Metabolic Intelligence app interprets your lipid panel as a complete metabolic profile, not a list of thresholds. Analyse your results at app.dafee.fr.